
Salena with Dr Paul Sugarbaker
Pseudomyxoma Survivor representatives once again attended the bi-annual Peritoneal Surface Oncology Group International (PSOGI) conference, this time it was in Paris. The PSOGI aims to “improve the treatment and survival of peritoneal cancer patients by educating patients, by training physicians, by organizing meetings and by performing basic and clinical scientific research into peritoneal cancer and the different treatment modalities”.
It is very much a conference aimed at developing and sharing best practice amongst the medical profession who deal with peritoneal cancers, of which ours is one. A record 800 people attended this time around, chances are your surgeon or at least a member of their team was there… and we tried our best to speak with most of them!

Susan with Dr Laura Lambert
We’ve asked them to help keep our database up to date and to continue to tell their patients about Pseudomyxoma Survivor and the work that we do. I met with some of our medical advisory panel including Professor Wim Ceelen at Ghent University, Laura Lambert, MD at the Huntsman Cancer Institute and Mr Faheez Mohamed from Basingstoke and they are delighted to continue working with us. We are now busy working behind the scenes to bring to fruition some projects they approached us about.
Professor Moroz, from Perth in Australia and Armando Sardi MD, Mercy Medical Centre – I didn’t manage to track you down but thank you for your continued support. I am also delighted that some other specialists have agreed to join our panel – more of which at a later date.
I was delighted that Pseudomyxoma Survivor was mentioned in a few of the talks and presentations, highlighting once again the positive working relationships we have within the community.
What can we take away from PSOGI 2018?

Susan with representatives from the nursing team form the Christie in Manchester
The consensus when I spoke to the medics was that some of the recent trial findings appear contradictory. For example, to HIPEC or not to HIPEC? Open surgery or laparoscopic? Perhaps we will have better clarity next time around. Some of the new developments sound really promising such as a direct injection of Bromelain and N-Acetylcysteine into recurrent pseudomyxoma peritonei of appendiceal origin – we await trial results.
What we can all agree on is that PMP has its own challenges including:
- Patients with PMP that cannot be cured by CRS-HIPEC do not have any efficacious treatment
- CRS-HIPEC is not available to all PMP patients
- PMP may be misdiagnosed and therefore not referred to CRS-HIPEC
- Rare disease (few cases, fragmented research effort)
European Network on Pseudomyxoma Peritonei
The European Network on Pseudomyxoma Peritonei or EuroPMP is a group which tried to get off the ground a few years ago but unfortunately lacked funding. This has now been resolved and their focus will be to link together all the experts in PMP research to improve standards of care for thousands of patients. Which is why we are thrilled to be recommended by Mr Faheez Mohamed from Basingstoke to be on the management committee of this interesting new group.
SQUEAMISH ALERT!
The videos I watched, of actual operations, showed an alien landscape which these medical professionals have made it their job to understand and navigate. I will admit, that during all my 5 operations, 3 rounds of chemotherapy and radiotherapy I didn’t consider the risks that the whole medical team could potentially be placing themselves in for me. When HIPEC is administered, for example, some agitate the drug inside you with their hands and can be up to their elbows in your innards. A sobering thought and quite a few of the presentations focused on the results of trials looking into the health and safety of the healthcare professionals. I’m relieved to say that if the recommended precautions are taken then there is little risk.
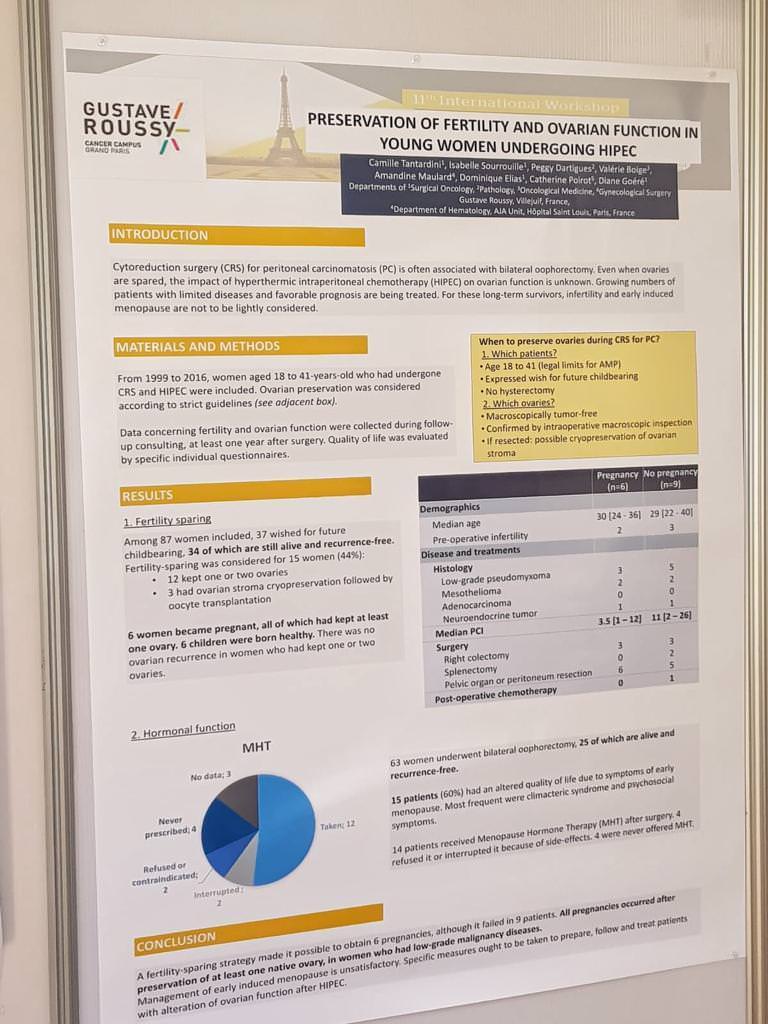
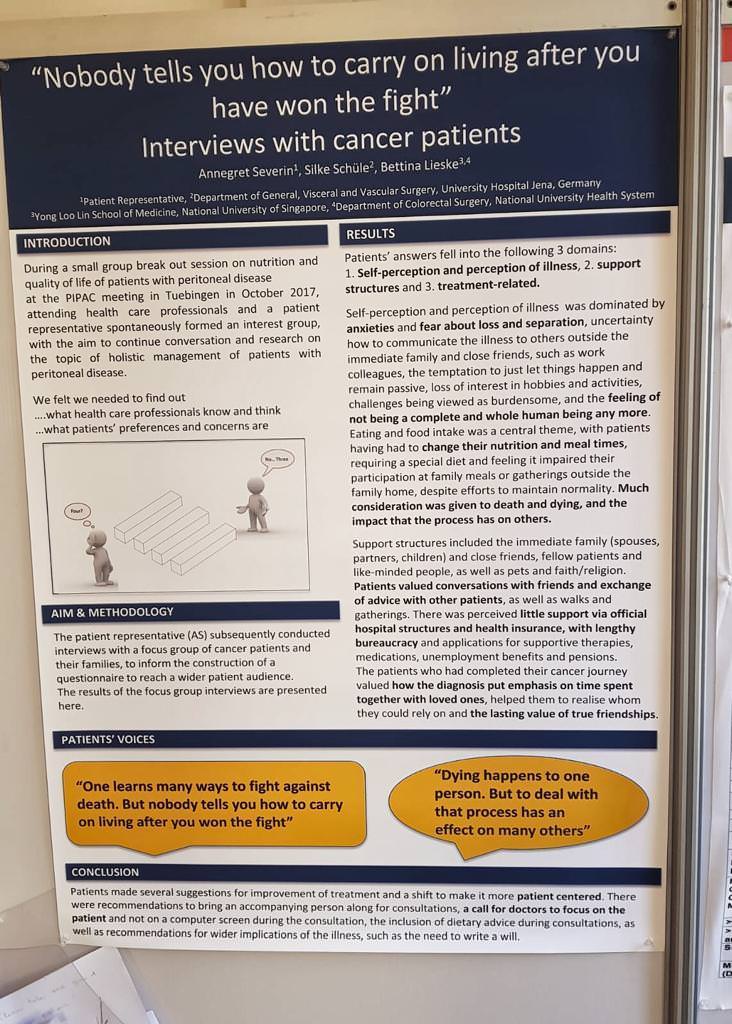
Back to safer ground now for me, I can report that quite a few of the presentations and posters, focused on the patient experience and voice. This focus helps to highlight the importance of patient groups such as ours and a shift to seeing the patient as a whole and not merely a ‘specimen’ on the operating table.
So much progress being made in the aims of the PSOGI – well done to all involved for the hard work being input. A special thank you to our own representatives and to you Susan for a very concise, detailed report of the Conference.
It’s really heartening to see all of the experts in one place and doing their bit to get the best medical advise to their patients June, I was really lucky to be a part of it on behalf of Pseudomyxoma Survivor.
THERE SEEMS TO BE A SIGNIFICANT ADVANTAGE IN THE U.S.A. FOR PMP PATIENTS AND SUVIVORS FOR PMP SPECIALIST SURGEONS WITH HIGH QUALITY MEDICAL CENTERS. AND, YET, MISDIAGNOSIS, AS IN MY CASE, SEEMS TO BE EVIDENT AT HOME AND ABROAD. C.T. SCANS WITH BARIUM CONTRACST SEEM TO BE THE MOST ACCURATE TO FIND PMP. IS THAT STILL THE CASE? THANK YOU FOR ALL YOU DO TO COORDINATE BASIC “HEADS-UP” AND HOPE FOR ALL AFFECTED BY PMP.
Hi Brian – sorry to hear about your misdiagnosis. PMP is rare and unfortunately, misdiagnosis is all too common – it’s one of the reasons why this charity was set up to try to address this. As I understand it MRI scans can give a very accurate picture but due to the costs involved are a secondary diagnostic tool after CT scans. Blood markers can also indicate if there is an issue but only if baseline levels are in your file to begin with. CT scans are the most common route to diagnosis. Thank you for your kind comments.